Article reviewed and approved by Dr. Ibtissama Boukas, physician specializing in family medicine
Arnold-Chiari malformation is a rare congenital or acquired malformation of the cerebellum that seems to affect more women than men. Although all populations are affected without distinction, it is often discovered by chance between the ages of 20 and 35 years. An individual can then live with the Arnold-Chiari malformation a lifetime without knowing it because it can be asymptomatic. But it can also manifest itself through multiple symptoms.
This popularized article will give a more precise definition of the Arnold-Chiari malformation, its symptoms and causes. It will also list the means of diagnosis and the means of treatment.
Go directly to the section that interests you
Definition
La Arnold-Chiari malformation is an abnormality due to the fact that the lower part of the cerebellum (cerebellar tonsils) engages in the foramen magnum called a large hole (hole located in the center of the vertebrae). So instead of the cerebellum resting on the base of the skull, its lower portion enters this foramen (hole) normally occupied by the brainstem.
A bit of anatomy
The cerebellum is located posterior to the brainstem, in the posterior fossa. The cerebellum is joined to the brainstem by three pairs of cerebellar peduncles:
the inferior cerebellar peduncles (restiform and juxtarestiform bodies), which join the cerebellum to the medulla oblongata.
the middle cerebellar peduncles (brachium pontis), which join the cerebellum to the annular pons.
the superior cerebellar peduncles (brachium conjunctivum), which join the cerebellum to the midbrain (upper part of the brainstem).
The brainstem is an element of the nervous system that is located between the brain and the beginning of the spinal cord, inside the skull. It consists of three distinct structures:
the medulla oblongata (which provides the junction with the cervical spinal cord)
the annular protuberance (or bridge)
the cerebral peduncles (connected to the hemispheres of the brain).
The brain, like the cerebellum, is made up of two lobes. There are also two cerebellar tonsils. These cerebellar tonsils are located in the anterior part of the underside of the cerebellum. They are closer to the foramen magnum and are related to the medulla oblongata of the brainstem.
Arnold-Chiari malformation is therefore characterized by cerebellar tonsils abnormally low pitches that engage through the foramen magnum. Because of this structural abnormality, the cerebellar tonsils interfere with the circulation of cerebrospinal fluid (CSF). This results in a collection of LCS in the meninges of the spinal cord and brain. This creates pressure on the brain and spinal cord resulting in hydrocephalus and intracranial hypertension (HTIC).
The different types of Arnold-Chiari malformation
Type I
We are talking about Arnold-Chiari malformation type I when there is a herniation of the cerebellar tonsils of more than 5 mm in the foramen magnum. A syringomyelia of the cervical or cervico-thoracic spinal cord can be observed. Also referred to as " ptosis of the cerebellar tonsils » greater than 5 mm. Furthermore, the term Ectopia is used if the tonsil herniation is between 3 mm to 5 mm. A ptosis of less than 3 mm is considered normal.
Type II
La Arnold-Chiari malformation type II corresponds to a malformation that extends to the structures of the central nervous system. We observe a descent of the cerebellar vermis (part that separates the two lobes of the cerebellum) and elements of the brainstem. The fourth ventricle (cavity inside the brain in which the CSF circulates) changes, the whole forming a pouch-like elongation. There is a modification of the osteo-dural structures (bone and dura mater) which reduce the dimensions of the posterior cerebral fossa. Arnold-Chiari malformation type II is most often associated with a spina bifida.
There are the Arnold-Chiari malformations type II and IV which are described. They are exceptional and more severe. These malformations are no longer encountered either because they are lethal or because detected on ultrasound before birth. In these cases, the parents generally resort to medical termination of pregnancy.
Symptoms of the disease
The clinical manifestations of Arnold-Chiari malformation are highly variable. However, not all symptoms appear in all people with this pathology. Many have only one to 3 symptoms. The possible symptoms in the Arnold-Chiari disease are the following.
headaches posterior (at the back of the head) and neck pain, nuchalgia (neck pain). These pains are reinforced during Valsalva maneuvers (exertion with the mouth closed) during coughing, defecation effort for example, etc.
Balance disorders in association with sensory and motor disorders which occur in such a way unilateral (one side only) and distal (of the extremities). These disorders can affect an upper limb or the hand.
achievement of cranial nerves (especially lower) and brainstem creating diplopia (sensation of seeing double), a nystagmus (involuntary eye movement), ataxia(lack of coordination of movements), a dysarthria (motor speech disorders), a dysphagia (difficulty swallowing). Involvement of the cranial nerves is linked to the compression of the structures at the level of the foramen magnum.
Swallowing and speech disorders (difficulty speaking).
Achievement of the lower limbs with paraparesis (mild difficulty in movement) and spasticity
Sphincter and sexual disorders
Other disorders sometimes associated with Chiari malformation include:
la scoliotic deformity which may precede the onset of neurological signs by several years
Studies have highlighted the frequency and potential aggravation of disorders such as: sleep apnea, respiratory arrest, syncope, even sudden death.
Causes
The causes of the occurrence of Arnold-Chiari malformation are theoretical. Three main theories are described:
Theory 1
Abnormal circulation of Cerebrospinal Fluid (CSF) would push the cerebellum out of the cranial box (hydrocephalus, intracranial hypertension...).
Theory 2
This is the most commonly accepted pathophysiological mechanism for the Arnold-Chiari malformation based on a reduction or absence of development of the posterior fossa. The undersized posterior fossa is poorly closed to ensure normal brain development. It can be of congenital or acquired origin.
Congenital causes are:hydrocephalus, craniosynostosis (sutures of the skull closing too soon), thehyperostosis (abnormal thickening of the bones), the rickets resistant to vitamin D and type I neurofibromatosis.
This is the tethered marrow theory. The abnormal anchoring of the spinal cord at the base of the spine generates the hernia and is also the source of other symptoms.
Diagnostic
THEmedical imaging is essential to confirm the diagnosis of Arnold-Chiari malformation. THE scanner in bone window allows the analysis of bone abnormalities of the cranio-vertebral junction.
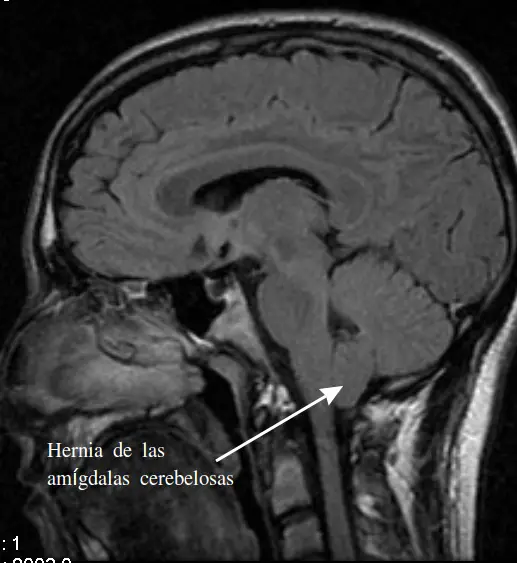
Magnetic Resonance Imaging (MRI) in sagittal section, associated with other incidences, allows a complete analysis of lesions, topographical relationships between the spinal cord and the other anatomical elements of the spine, fluid and vascular compartments.
Treatment
surgery
The only known treatment for Arnold-Chiari malformation is surgery. The decision to operate is made by a neurosurgeon taking into account the fact that the symptoms are indeed due to the Chiari malformation.
Surgery is only considered if the symptoms are sufficiently disabling. The objective of this surgery will be to lift the compression of the posterior fossa to free up enough space around the malformation. This will allow the Cerebro-Spinal Fluid to regain normal circulation and thus reduce or at least stabilize neurological disorders.
The different stages of this surgical procedure include, depending on the case:
A craniectomy: opening of part of the cranial vault
A laminectomies : removal of part of one or more vertebrae
A duroplasty (plasty of the dura mater): incision of the dura mater and placement of a patch to widen it.
Tissue removal : cerebral tonsils are sometimes cauterized
Closure of the cranial vault
No specific treatment forsyringomyelia (if associated) because it is a consequence of CSF circulation disorders.
After the operation, a re-education may be necessary and must be supervised by specialized nursing staff.
Pain management
Analgesics can be administered: levels 2, morphine derivatives.
La Transcutaneous Electrical Neuro Stimulation (Tens)
Hypnosis, acupuncture, physiotherapy
Management of other symptoms
A urinary catheter can be placed in case of urinary incontinence
Specific medications can be given to treat sexual impotence
Speech therapy sessions can help preserve phonation and swallowing
Physiotherapy (physiotherapy), balneotherapy and massage exercises can be useful to preserve maximum mobility of the arms and hands as well as walking
Psychological support could be considered
Conclusion
La Arnold-Chiari malformation is a congenital or acquired malformation of the cerebellum due to herniation of the tonsils of the cerebellum into the foramen magnum.
Types I and II are the best known and can be asymptomatic or symptomatic. The clinical manifestations of Arnold-Chiari malformation are multiple which makes the diagnosis not obvious.
Medical imaging, mainly MRI, confirms the diagnosis. The fundamental treatment to remove the malformation remains surgery. In addition, treatment of pain and other associated symptoms is necessary.
If you liked the article, please share it on your social networks (Facebook and others, by clicking on the link below). This will allow your relatives and friends suffering from the same condition to benefit from advice and support.

")
")
")
")


")
