Nearly 10 out of 100 adolescents suffer fromslipped capital femoral epiphysis. It's about a hip disease which mainly affects children and adolescents of growing age. It is also called " coxa vara ". What is the coxa vara? What are its causes ? How does it manifest? What does his treatment consist of? Find the answers in this article.
A few words about the coxa vara
Coxa vara most often occurs between the ages of 10 and 16. During this period, the bones undergo rapid growth.
Adolescents have a growth plate just below the femoral head epiphysis. This plate is called the “cervicocephalic growth cartilage”. The latter connects the femoral head and the femur. It is thanks to the cervico-cephalic growth cartilage that the bone can lengthen and develop.
The coxa vara therefore corresponds to a growth plate disease. This results in the slippage of the femoral epiphysis relative to the neck of the femur. The sliding can be sharp and brutal.
This hip disorder affects more boys than girls. In 80% of cases, it affects a single hip. It is bilateral without one in five cases.
Causes of this hip disorder
Slipped capital femoral epiphysis can be of genetic or acquired origin.
When the cervico-cephalic growth cartilage is abnormal, it becomes fragile and promotes sliding.
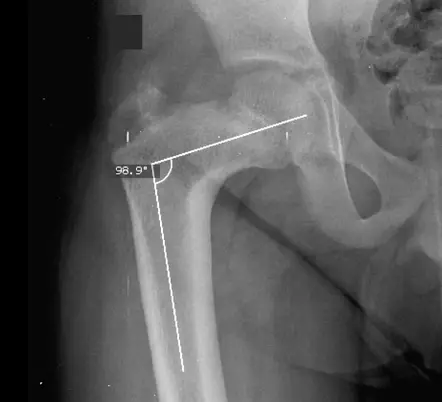
The deformation of the upper part of the femur can also be linked to the closure of the cervico-diaphyseal angle (angle of inclination of the neck of the femur and the body of the femur). This angle normally measures between 120° and 135°.
Due to the prevalence of this disease in boys, mechanical and hormonal factors may be associated with it. Slippage of the epiphysis can result from mechanical stresses exerted on the upper end of the femur. These stresses are sometimes exaggerated by trauma.
Also, cases of coxa vara are frequently observed in cases of overweight. The overload puts pressure on the growth plate, causing the femoral epiphysis to slip.
As part of this cartilage disorder, certain risk factors have been identified:
- endocrine disorders such as diabetes, thyroid disease or growth problems;
- kidney disease;
- cancer treatments such as chemotherapy or radiotherapy;
- taking certain medications such as steroids;
- family history.
What are the symptoms of this disorder?
The coxa vara symptoms reflect the amount of slippage.
The disease is mainly manifested by a hip stiffness. The child may feel pain in the fold of the groin without having suffered trauma. The pain may radiate to the antero-medial part of the thigh to the knee. Its intensity is variable: it can cause less lameness or an inability to walk.
Groin pain does not necessarily show up early on. It may happen that the child feels pain directly in the knee or thigh. If nerves are irritated, the pain may affect an area other than the hip.
A trauma can lead to complete functional impotence as well as a vicious attitude in external rotation of the lower limb.
The child may have other signs:
- limited hip movement (in rotation, flexion and abduction);
- difficulty turning the toes inward;
- avascular necrosis (death of bone tissue) with collapse of the epiphysis;
- pain on movement.
In more severe cases, epiphysiolysis leads to early coxarthrosis (hip osteoarthritis). The risk is high when the slip is below 40°.
Slipped capital femoral epiphysis diagnosis
Le clinical diagnosis of coxa vara is often confirmed by an X-ray. This examination detects the suggestive signs of the disease and shows the appearance of the coxo-femoral joint.
The x-ray requires two correct views, in particular a view of the pelvis in standard front view and a view of each hip in profile view. The profile incidence is the most relevant. It makes it possible to analyze the rocking of the epiphyseal nucleus inwards and backwards.
The doctor often uses Dunn's technique. For this, the patient must do:
- 90° flexion;
- abduction so that the cervix is parallel to the plate;
- internal rotation corresponding to anteversion.
Sometimes the doctor orders additional tests such as an ultrasound or magnetic resonance imaging (MRI). MRI sometimes requires the use of a contrast product. Introduced intravenously, it can highlight the structures of the hip. MRI helps determine the severity of femoral head necrosis, and can also help guide treatment.
What can be done to treat this joint disorder?
Le coxa vara treatment is primarily surgical. The operation is performed under general anesthesia.
Coxa vara is a progressive disease. In other words, it requires an operation as soon as it is diagnosed. The surgical intervention restores the angle between the diaphysis (body of the femur) and the neck of the femur. It also limits the risk of avascular necrosis of the hip.
Once the diagnosis has been made, total rest is recommended until the day of the operation. The child must be admitted to the hospital urgently to ensure rest and to plan the intervention as soon as possible. Weight-bearing is thus contraindicated: it accentuates sliding and constitutes a poor prognosis.
For less severe cases
When the condition is mild, the operation consists of fixing the femoral head “in situ”. For this purpose, the surgeon uses a screw to limit slippage. The procedure is monitored using a fluoroscope. It is a radioscopy instrument that shows images in real time.
The surgeon makes an incision near the hip, then passes a metal screw through the femoral bone and growth plate. The goal is to hold the femoral head in place. Normally, the patient does not feel this screw after the surgery.
In those who have both hips affected, it is possible to stabilize them. This decision can be made even if signs of disease on the other side of the hip have not yet appeared.
For more severe cases
When the coxa vara is more severe, the intervention is more complex. The femoral head should be realigned to the same level as the femoral neck. To do this, the surgeon must access the inside of the hip joint. The objective remains the same: to maintain the femoral head with a screw. The intervention also makes it possible to minimize the risks on the vessels which vascularize the femoral head.
After the operation, the child is followed by a medical team. This indicates the weight that can be applied to the operated leg. The follow-up must be regular and be done every 3 to 6 months until the end of the growth.
Following the operation, children who have had both hips operated on may need a wheelchair to get around for the first two weeks after the operation. For less complex cases, the use of a cane for around 6 weeks may be recommended.
Finally, coxa vara develops favorably when diagnosed and treated in time. Children who suffer from moderate and severe epiphysiolysis are at greater risk of joint problems. This can be a difference in leg length or osteoarthritis. In this case, further surgery could be considered.
Projects

My name is Arotoky and I am studying human medicine. Web editor for more than 5 years, I currently focus on the theme of health and well-being. I have the strong conviction that with my valuable articles, I can help many people to relieve their ailments and feel better. My goal is to share my health knowledge with the general public through web writing.
")
")



")