
Your doctor has diagnosed you with a narrow spinal canal (also called spinal canal narrowing or stenosis). Apparently, this diagnosis is responsible for your back pain.
What is narrow lumbar canal, and how does it manifest? Should we be worried? Are there natural remedies or treatments that are less invasive than surgery?
In this article written by a physical therapist, we discuss narrow lumbar canal in detail with a focus on natural solutions to reduce your symptoms. As a bonus, we will share exercises to relieve you.
Definition and Diagnosis of Narrow Spinal Canal
A mini lesson in anatomy will help you better understand the diagnosis of narrow lumbar canal.
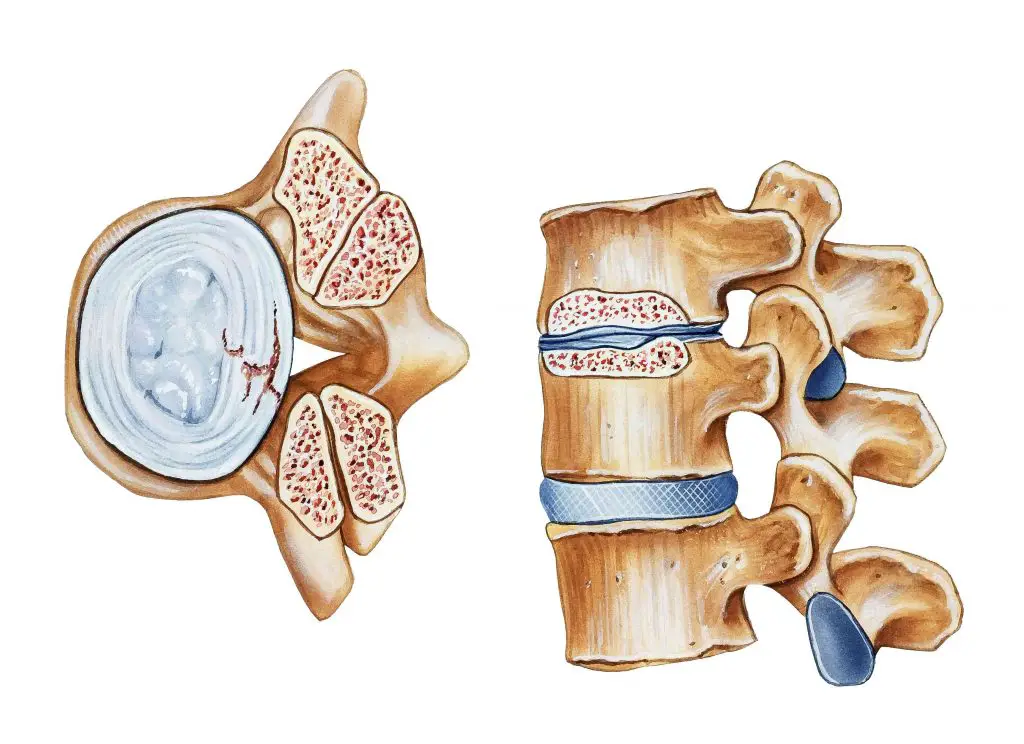
The spine (or spine) is composed of superimposed vertebrae. In the lumbar region (lower back), there are 5 vertebrae which we call L1, L2, L3, L4, and L5. There is a hole between each vertebra called the vertebral foramen.
The juxtaposition of the vertebrae (via the intervertebral discs and zygapophyseal joints) forms a canal called the spinal canal. This is where the spinal cord passes and from where the nerve roots originate (which give, for example, the sciatic nerve or crural nerve).
In the narrow lumbar canal, the size of this Spinal canal decreases at the level of the lumbar vertebrae (L1 to L5). Normally this canal is around 15mm in diameter, but it is considered "narrow" when it is less than 13mm.
But why is the canal narrowing, you ask me? The causes are multiple and depend on each individual.
Here are the most common:
Lumbar osteoarthritis
Because it is often associated with osteophytes (bony prominences), lumbar osteoarthritis often results in a decrease in the size of the spinal canal. This degenerative cause is the most common of narrow lumbar canals.
This is also the reason why the population concerned is often over 50 years old.
To know everything about lumbar osteoarthritis, see the following article.
Spondylolisthesis
Le spondylolisthesis refers to a slipped vertebra. Inevitably, this will reduce the size of the spinal canal, and could lead to a narrow spinal canal.
Herniated disc
If the disc migrates backwards due to a herniated disc, it will reduce the size of the spinal canal and thus lead to a narrow lumbar canal.
Congenital
As mentioned, the normal diameter of the vertebral foramen is approximately 15 mm. Some people are born with a smaller spinal foramen.
They will therefore be at greater risk of developing a narrow lumbar canal in the future in the event of osteoarthritis or other conditions reducing the circumference of the spinal canal.
Other experience
Any pathology or condition that causes a reduction in the size of the spinal canal can lead to a narrow lumbar canal.
We think, among other things, of the following conditions:
- abscess
- infections (such as spondylodiscitis)
- you die
- hematomas
- yellow ligament hypertrophy
- etc.
Diagnosing a narrow lumbar canal
Concretely, how can we differentiate between the various causes of narrow lumbar canal?
It is often the clinical examination and medical imaging that will determine the potential cause of the narrow lumbar canal.
A doctor (or other back specialist) will perform a complete medical examination taking into consideration your medical history, and your associated conditions. Then he will do certain movements and other tests to identify the cause of your back problem.
Certain imaging tests will help clarify the diagnosis. There radiography will confirm the existence of the narrow lumbar canal, and will determine whether there is osteoarthritis or spondylolisthesis.
A magnetic resonance imaging (MRI), for its part, will provide information on the integrity of nervous structures, discs, etc.
What's more, un electromyogram (EMG) could also be prescribed to better appreciate nerve conduction in the legs.
Anyway, the narrowing of the lumbar canal sometimes comes with its share of consequences, especially when we know the importance of the anatomical structures that pass through the spinal canal (such as the spinal cord, nerves, blood vessels, etc. .).
Concretely, how does the narrow lumbar canal manifest in an individual? This is what we will discover in the next section dealing with the symptoms of this condition.
What are the symptoms of narrow lumbar canal?
What if I told you that the narrow lumbar canal was sometimes asymptomatic? In fact, according to some studies, up to 28% people with a narrowed lumbar canal on medical imaging did not present with lumbar pain.
On the other hand, it often happens that a narrow lumbar canal causes symptoms. This will depend on certain factors such as the narrowing itself, and also the irritated structures.
The most common symptom is low back pain (pain in the lower back).
As the narrow lumbar canal causes narrowing of the spinal canal, this can cause irritation to the surrounding nerve structures. If the nerves are irritated, neurogenic symptoms such as sciatica ou cruralgia (such as pain irradiations behind the thigh or Calf, tingling, numbness, etc.).
This condition can also cause weakness and muscle fatigability of the limbs, leading to pain. general fatigue and the need to stop walking after short distances.
In severe cases, there may be a cauda equina syndrome.
What is a ponytail? These are nerve roots located in the lower back that emerge from the spinal cord and provide control to the lower extremities and organs located in the pelvic region.
At this time, anesthesia around the genital area, sphincter disorders (urinary and fecal incontinence), erectile dysfunction, and/or flaccid paralysis of the lower limbs will be observed. This is a medical emergency which sometimes requires surgical intervention!
Another potential symptom of narrow spinal canal is intermittent claudication. In addition to low back pain and pain in the lower limbs, the patient's complaints may be a feeling of heaviness in the legs, muscle fatigue and night cramps.
Typically, symptoms are worse on walking, and relieved on sitting. This comes from the fact that the lumbar flexion (as in a sitting position) momentarily increases the size of the lumbar canal, while extension and maintained lumbar lordosis (as in walking – especially when descending a slope) narrows it.
This is also the reason why people with narrow spinal canal find their symptoms ease when they lean on a grocery cart in the supermarket. This is the “Caddy sign”.
Narrow lumbar canal treatments
Treatment generally begins with so-called “conservative” methods to relieve the condition naturally. Unfortunately, some situations require more invasive interventions.
In general, treatment includes:
Medication
Although it won't correct the cause of the narrow spinal canal, medication can be helpful in controlling the symptoms.
The doctor often starts with a prescription for anti-inflammatory, painkiller and/or muscle relaxants to control the initial symptoms.
In the case of neuropathic pain (for example, radiation in the leg associated with numbness and tingling), the doctor may prescribe anti-epileptic drugs such as Lyrica.
In cases of severe pain, it is possible to resort to anti-depressants, oxycodone, codeine, morphine and its derivatives, etc.
Note: It is imperative to follow your doctor's recommendations regarding your medication. He will know how to choose the right medications and adjust the doses based on your medical history and general health.
Rest and lumbar support
Please note, do not confuse relative rest and complete bed rest. The mistake many people with low back pain make is to stay in bed until the low back pain subsides.
Although this can relieve symptoms, this strategy comes with its share of consequences, such as increased stiffness, muscle atrophy, social isolation, and so on.
The best solution will therefore be to minimize rest as much as possible, and instead limit movements that accentuate the pain.
For example, a therapist might ask you to temporarily avoid swimming and any other activity involving lumbar extension movements. Or, the walking periods could be limited to a certain time so as not to aggravate the symptoms.
In more extreme cases, a doctor might prescribe a lumbar corset that would limit lumbar hyperlordosis. Again, don't get used to wearing the brace long term, and wear it more like a crutch that you would use after a sprained ankle. The same is true for the lumbar belts.
Massages and manipulations
Since narrow spinal canal is most often accompanied by lower back pain, manual techniques from a therapist can help.
Massages or mobilizations from a osteopath, physiotherapist (physiotherapist) or chiropractor can thus reduce pain and reduce associated muscle tension.
On the other hand, these methods alone are not sufficient in the long term, and should ideally be accompanied by a active approach.
Active approach (physiotherapy)
It is sometimes difficult to conceive that exercise can help relieve back pain, especially when all movements are painful.
On the other hand, the scientific studies are unanimous: Physical exercise is the best way to combat low back pain in the long term.
Obviously, you need to be active in a safe and progressive setting when you suffer from lower back pain, and the physiotherapist (physiotherapist) is the therapist of choice to guide you.
Alternative treatments
Alternative treatments and natural products certainly have their place in the management of the narrow lumbar canal, but their limits must first be identified.
No, an acupuncture session will not correct the source of your narrow spinal canal. Nor even the cupping, Shiatsu-massage, medicinal plants, etc.
These modalities will rather act on the consequence of your lumbar canal (such as pain and/or lumbar stiffness), and offer you often temporary relief.
If the pain prevents you from going about your business, and you prefer to limit the intake of medication, these treatments can be effective in addition to a medical approach to improve your quality of life.
Other forms of alternative medicine sometimes used in the treatment of narrow spinal canal include:
- acupressure mat
- myotherapy
- Quinton plasma
- percutaneous hydrotomy
- therapeutic yoga
- craniosacral therapy
Natural remedies that may relieve symptoms include (click on the product you are interested in for purchasing options):
Turmeric
Thanks to its antioxidant and anti-inflammatory powers very powerful, turmeric is one of the most used plants in a culinary and therapeutic context. The composition of turmeric is essentially made of essential oils, vitamins (B1, B2, B6, C, E, K) and trace elements. But it is to its composition rich in curcumin and curcuminoids that we owe them and calm skin of this spice.

- Turmeric Capsules with Black Pepper – Turmeric is known for its healing properties…
- Turmeric Capsules Rich in Vitamins and Minerals – Turmeric is an excellent source of…
- Alternative to Turmeric Powder – These turmeric capsules are multi-purpose, they…
Last updated on 2025-07-01 / Affiliate links / Images from the Amazon Partners API
Ginger
In addition to the particular flavor it brings to cooking and its aphrodisiac properties, ginger is a root well known for its anti-inflammatory powers. THE gingerol gives it its anti-inflammatory action. It is an active component acting on the inflammatory pain related to chronic joint inflammatory diseases, including rheumatoid arthritis, lupus, rheumatic diseases, etc. It has been proven that this active element is also effective in acting on the inflammation linked to arthritis and sciatica. Ginger also has other benefits thanks to its high potassium content and its richness in trace elements (calcium, magnesium, phosphorus, sodium) and vitamins (provitamin and vitamin B9).

- 【Natural Ginger Foot Patches】: Natural Foot Detox Patch with Ginger and…
- 【Ginger Anti Swelling Detox Patch】: Ginger Detox Patches are natural,…
- 【Removes Body Toxins】: Ginger Foot Patches helps reduce the buildup of…
Last updated on 2025-07-01 / Affiliate links / Images from the Amazon Partners API
Omega-3
Omega-3s are polyunsaturated fatty acids that play a very important role in the functioning of our body. They are provided by food in three natural forms: docosahexaenoic acid (DHA), alpha linolenic acid (ALA) and eicosapentaenoic acid (EPA). Beyond their action on the brain and the cardiovascular system, omega-3s prove to be very effective against inflammation. Indeed, they have the ability to act on the inflammatory mechanisms in osteoarthritis by slowing down cartilage destruction, thus they reduce the intensity of osteoarthritis pain. Sciatica, being most often linked to an inflammation secondary to a herniated disc, it can also respond to omega-3 provided it is consumed regularly.

- ✔ WHY NUTRAVITA OMEGA 3 FISH OIL? – Our Omega 3 Fish Oil is naturally sourced from the rich waters of the Peruvian coast. The oils are then distilled for increased purity to provide the highest levels of contaminant-free Omega 3 fatty acids – EPA and DHA, removing metals, PCBs and other toxins. At 2 capsules per daily serving, our supplement provides a maximum strength of 660 mg of EPA and 440 mg of DHA. You also get 240 capsules per bottle for a 4 month supply.
- ✔ WHY OMEGA 3? – Each recommended daily dose of our premium Omega 3 fish oil supplement provides high-potency essential fatty acids – Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) both contribute to the maintenance of various bodily functions, most importantly the normal functioning of the heart. DHA, on the other hand, supports the maintenance of normal brain function and normal vision. All claims are substantiated by EFSA (European Food Safety Authority).
- ✔ 3RD PARTY LAB TESTED – Each ingredient is quality tested before the manufacturing process begins, each batch of our supplement undergoes rigorous quality testing. Our products have been third party tested for heavy metals and unwanted compounds by one of the best testing centers in Europe, the lab is Ukas accredited to ISO/IEC 17025:2017 standards. The results are then analyzed and certified by another top lab.
Last updated on 2025-07-01 / Affiliate links / Images from the Amazon Partners API
Lemon eucalyptus
Eucalyptus is a plant most often used in the form of herbal tea or essential oil. She would have anti-inflammatory effects which give it the ability to act on the bone and joint pain in general and the pain of sciatica in particular.

- Eucalyptus Citriodora Essential Oil.
- 100% pure.
- Botanical name: eucalyptus citriodo.
Last updated on 2025-07-01 / Affiliate links / Images from the Amazon Partners API
wintergreen
Wintergreen is a shrub from which a very interesting essential oil is extracted. It is one of the essential oils most used in aromatherapy. This oil, extracted from the shrub of the same name, is used in massage to relieve sciatica and act like a analgesic. Indeed, it provides a heating effect thanks to its ability toactivate blood circulation locally.

- PROPERTIES ORGANIC WINTERGOOD ESSENTIAL OIL: Wintergreen essential oil is…
- DIRECTIONS FOR USE: Refer to the instructions or ask your pharmacist for advice, This…
- PURESSENTIEL DNA: A range of 55 essential oils essential for well-being in the…
Last updated on 2025-07-01 / Affiliate links / Images from the Amazon Partners API
Note: Remember that these products do not replace medical treatment. Do not hesitate to consult for support adapted to your condition.
Adaptation of the workstation
Certain professional activities carry risks for the back. We are thinking, among others, of delivery men, cleaners, truck drivers, etc.
In other words, tasks involving repetitive motions, heavy lifting, and/or prolonged static postures can increase back pain.
If your symptoms seem to get worse after a day's work, your doctor may grant you a variable length of time off work. Similarly, a job adaptation could help you.
Un Occupational therapist is a professional of choice to adjust your screens, show you optimal load handling techniques, propose a gradual return plan after a shutdown, etc.
In extreme cases, the retraining or professional redeployment can be considered.
Weight loss
In theory, the weight loss may have a positive effect on narrow spinal canal symptoms through the following mechanisms:
- Reduced stress on the lumbar intervertebral discs, thus preventing the development or aggravation of a herniated disc.
- Reduced stress on the posterior vertebral (facet) joints, thus preventing the aggravation of lumbar vertebral osteoarthritis.
- Facilitation of spinal movements.
Even if the results differ from one person to another (depending on the severity of the narrowing, the cause, the terrain…) and are not guaranteed, it would be a shame not to try to lose a few pounds and then reassess their symptoms.
It is not always easy to lose weight when you suffer from a narrow spinal canal. The pain and other symptoms it generates sometimes discourage any physical activity.
However, it is important to ensure that you maintain a certain degree of daily activity to lose weight, or at least stabilize your weight and avoid joint stiffness.
In addition to physical activity, it is recommended to adopt a balanced and varied diet. the anti-inflammatory diet is particularly valuable in this context, as it helps provide the body with all the nutrients it needs while reducing inflammation throughout the body. It therefore allows weight loss and a reduction in pain of inflammatory origin.
Infiltration
The doctor may suggest infiltrations to relieve the pain, especially when the medication does not seem to have an effect.
In general, the doctor goes there from one lumbar cortisone infiltration (depending on levels and irritated structures) Ideally, ultrasound-guided infiltration should be used to maximize results.
To learn all about infiltration (including the risks and benefits of each type of infiltration to relieve your symptoms), see the following article.
How to sleep with a narrow lumbar canal?
It is not uncommon for people diagnosed with a narrow spinal canal to complain of poor quality sleep.
With this in mind, here are some sleeping postures that are sometimes effective in relieving symptoms and sleep better at night.
Lying on your back with a pillow under your knees
This position reduces the anteversion of the pelvis (lumbar hyperlordosis), which reduces stress on the facet joints. Basically, keeping your knees slightly bent will prevent your back from arching excessively, reducing the stress on your vertebrae.
For people who see their symptoms worsen in extension (often the case in the presence of a narrow lumbar canal), this position can be comfortable and thus improve the quality of sleep.
Lying on your side with pillow between your legs
Keeping a pillow between the legs reduces lumbar torsion. By bending the knees, this also decreases the lumbar lordosis (sometimes painful in the presence of a narrow lumbar canal).
For more comfort, many people opt for a knee pillow such as this one.
Everything you need to know about narrow lumbar canal surgery
Unfortunately, some people with a diagnosis of narrow lumbar canal will sometimes need to resort to the operation to relieve their symptoms.
When to consider surgery?
Remember that this treatment option should not be considered straight away. On the other hand, we will consider surgery in the following situations:
Red flags
Some conditions require urgent medical (and often surgical) intervention. This is particularly the case of cauda equina syndrome previously discussed.
Symptoms are often severe and disabling.
Persistence of pain
Sometimes the lumbar canal causes a persistent functional disability. In other words, it greatly affects the quality of life of the sufferer.
In the event of persistent disability (between 3 and 6 months) despite well-conducted conservative treatment, a medical specialist may consider the surgical option.
What types of operations are possible?
Once the doctor has decided that surgery is the preferred option to treat the narrow spinal canal, the goal will be to increase the size of the spinal canal.
This involves correcting (or removing) the structures that narrow the spinal canal. The decompression laminectomy, where surgical removal of the spinous process and vertebral laminae is performed, is often used.
When the stability of the vertebrae is compromised (for example, a spondylolisthesis in advanced stage), arthrodesis can be performed. This consists of a surgical fusion of 2 vertebrae to increase stability.
Obviously, an orthopedic surgeon will discuss with his patient the types of surgery possible, the associated risks, the prognosis for recovery, etc. More and more orthopedists are using endoscopic surgery to minimize complications and speed healing.
Other types of decompressive surgery
Other types of decompressive surgeries include:
- Laminoplasty
- Discectomy
- Corpectomy
- Foraminotomy
- Flavectomy
It should be noted that the optimal surgical technique for treating the spinal compression or nerve roots remains controversial. One approach is not necessarily superior in all circumstances, and the best option will depend on patient-specific anatomical and symptomatic factors.
What convalescence following a narrow lumbar canal operation?
Recovery following a narrow spinal canal operation will depend on several factors.
On the one hand, the type of surgery will influence the prognosis for recovery. If the surgeon had to install rods and screws, the healing time will necessarily be longer.
If he opts for a laminectomy, we can hope to walk again the next day after the operation. Obviously, a physiotherapist or nurse will guide you in this process.
The duration of hospitalization lasts an average of 3 to 5 days. This will allow the medical team to provide you with post-operative care, to monitor and detect complications (rare), and to prepare for your discharge.
In general, the patient is returned home after the hospitalization period. In some cases, a convalescent home may be considered before returning home. You will need to discuss your specific situation with the surgeon.
The work stoppage will generally last between 6 to 12 weeks depending on your situation (job, medical condition, rehabilitation, etc.). A physiotherapist and/or an occupational therapist will support you in your return to normal life (home chores, work, sports activities, etc.)
Conclusion (the take-home message)
I hope you are now more familiar with narrow lumbar canal if your doctor has ever given you this diagnosis.
More precisely, you have an idea of the different possible causes of narrow lumbar canal, and also know the symptoms according to the anatomical structures affected.
As for the treatment, remember that it should start with so-called conservative methods with the aim of avoiding surgery as much as possible. Passive treatments can relieve you, but don't forget to complement them with an active approach.
In extreme cases, surgery remains a viable option. An orthopedist will know how to weigh the pros and cons of surgery based on the symptoms and their implication in the patient's life.
Good recovery!